Mind the Gap & Why ‘Ruby’s Rule’ Won’t Work.

Ruby Yen Chan, a 3 year old from Queensland, died from an air embolus. You can read the coroners report here.
The process of disconnecting an intravenous fluid bag allowed air to enter it. When the bag was later re-connected (re-spiked) the air passed through the intravenous line and into Ruby’s circulation leading to her death.
The coroner’s recommendations focused on outlawing the practice of IV fluid bag re-spiking:
While we strongly support ‘Ruby’s Rule’ we recognise it will do little to stop the same adverse event from happening again.
IV fluid bag re-spiking occurs every day in hospitals throughout the world.
This is ‘The Gap’ that exists between work as perceived by managers and work as performed by front line staff.
Many hospital staff haven’t heard of Ruby’s Rule, and even those who have continue to re-spike bags for numerous reasons – understanding these requires an understanding of the complexity of our work environments.
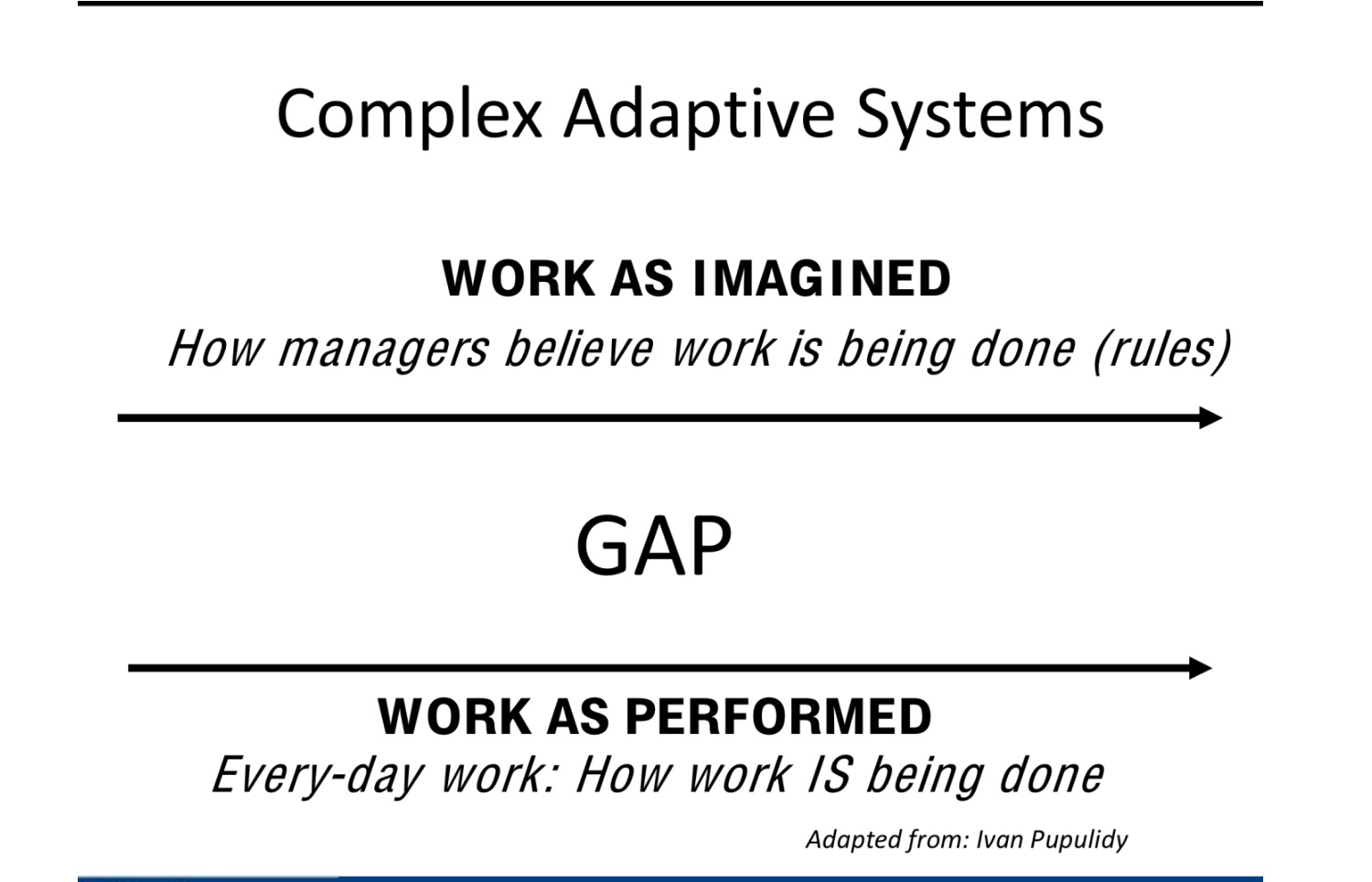
This gap is endemic to top down safety approaches.
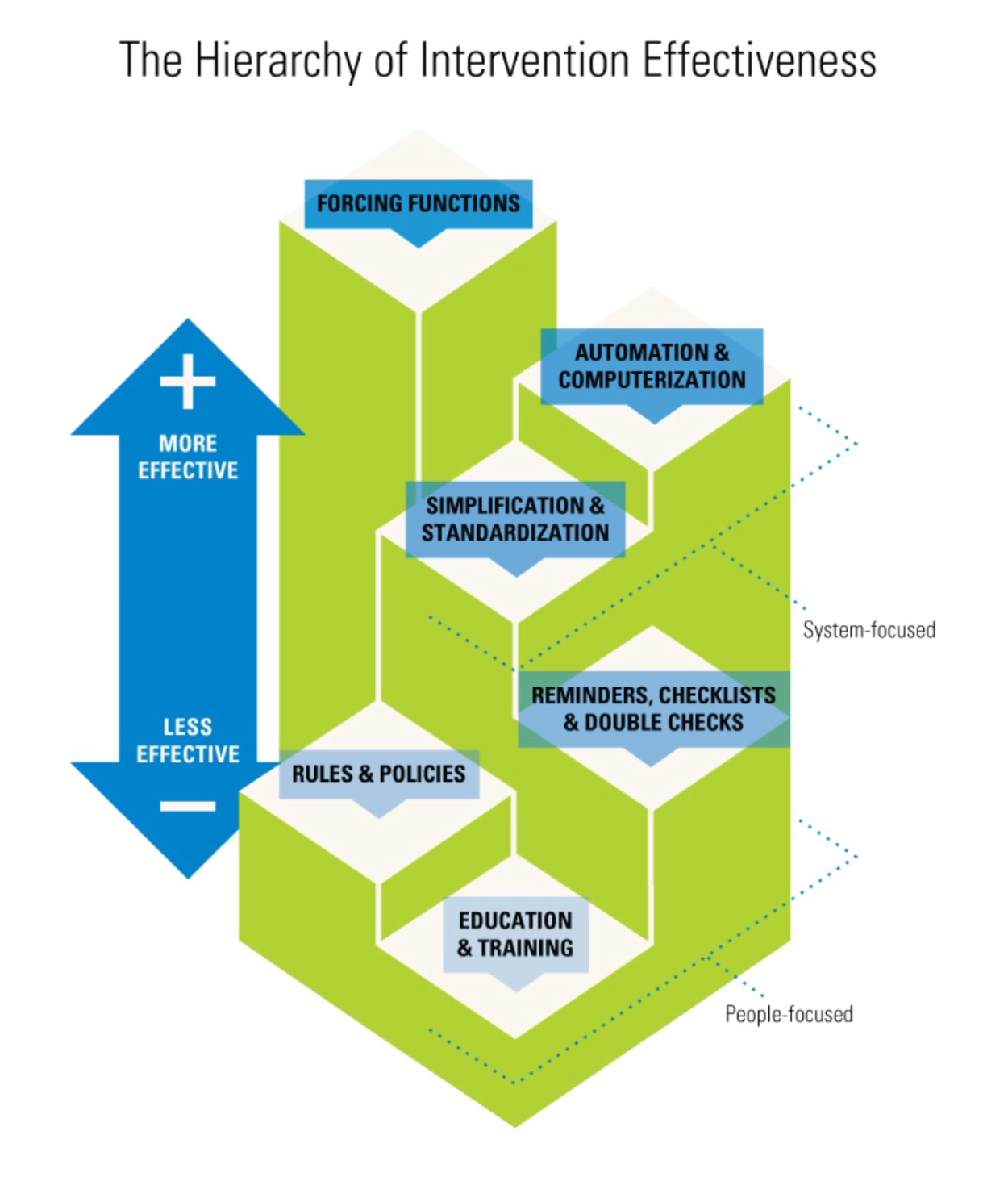
Fortunately a highly effective solution to this adverse event already exists on the front line.
It’s not the re-spiking that’s the issue – it’s that air enters the IV fluid bag on disconnection. If we can stop air entering the fluid bags then problem solved – this is a forcing function and is a highly effective safety measure:
IV fluid bags with valves which prevent air entrainment (on right in image below) are already in use in many hospitals.
Click on image for video:

Preventing future similar events would require replacement of all non-valved IV fluid bags with valved ones – at a cost saving of 1c per bag.
In Australia, the Therapeutic and Goods Administration (TGA) are best placed to effect this. We encourage them to do what’s best for patient safety.
We strongly support increased transparency in our error reporting systems so front line staff can develop effective safeguards.
(PatientSafe has no financial interest with any products discussed on this website)
2 Comments