
One major objective of a ‘Root Cause Analysis’ is to: ‘Look for improvements rather than apportion blame’
Recently, a tragic gas pipeline crossover resulted in death of a newborn, and left another with severe brain injury.
Prior to this incident many clinicians believed pipeline errors had been relegated to history. Unfortunately pipeline crossovers occur with relentless frequency (see here) – the RCA team may not have appreciated this. This affects the focus of their report – instead of finding solutions for preventing similar adverse events in the future they look at what could have stopped it in the past – a subtle difference and consequently the RCA recommendations appear like veiled forms of blame:
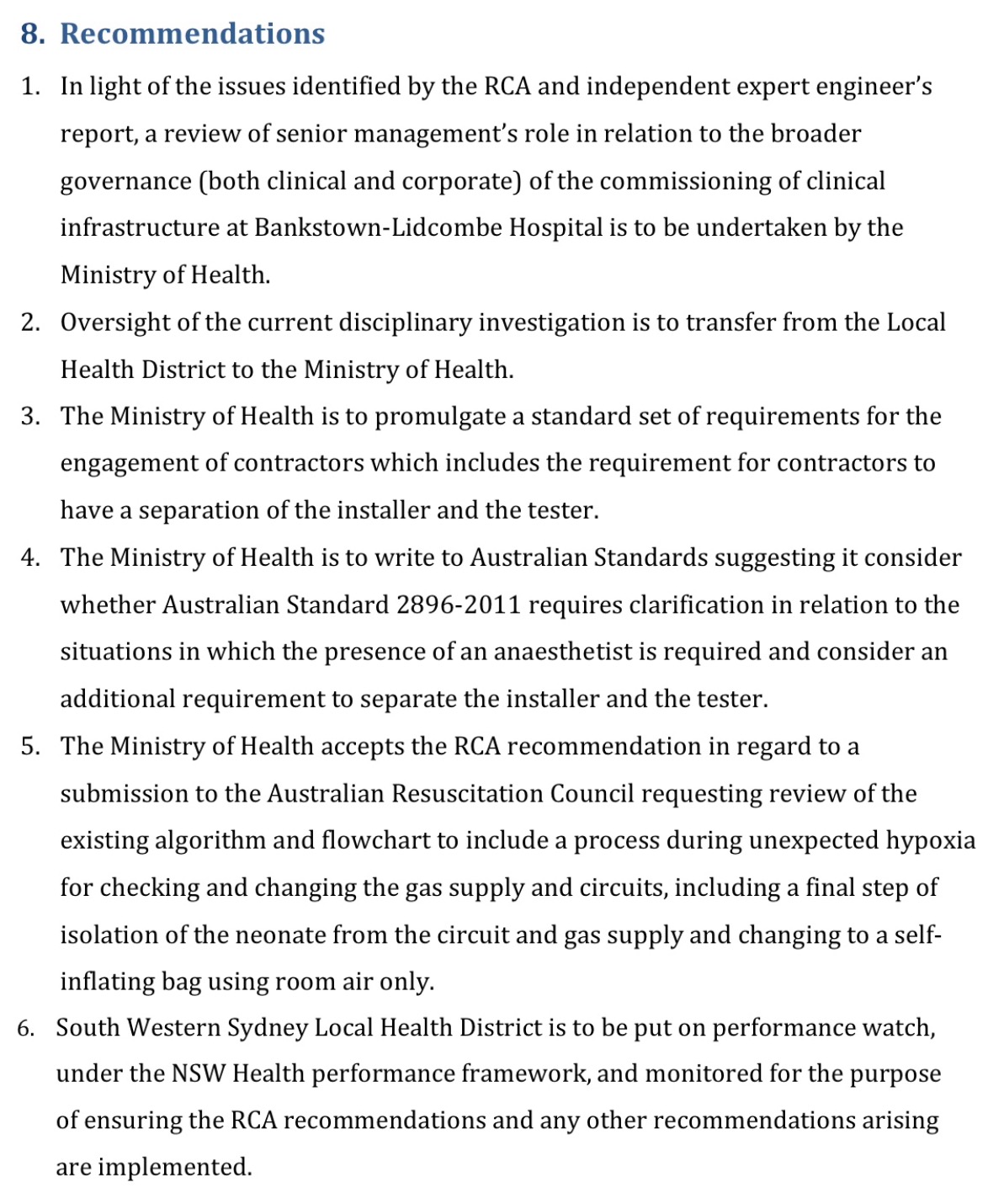
Blame seems to be directed towards senior management, the local health district, and contractors.
While prudent to review Australian Standards (recommendation 4) it’s wise to consider after years of pipeline crossovers further refinements to standards may have limited effect.
As a clinician recommendation 5 is of particular concern. There are multitude more common reasons for hypoxia in a newborn. One can only imagine the stress, in this situation, with removing a newborn from what is believed to be oxygen? Newborns are initially resuscitated using room air. They’re administered oxygen if they deteriorate – it would be unrealistic to expect a clinician to remove oxygen for the same reason they’re administered it. Perhaps it would be wise to assess through simulation how many ‘humans’ will actually do this. If recommendation 5 is adopted it will only serve to apportion more blame on the clinician – the ‘second victim‘.
Along with the RCA, there was significant media focus on blame. The health minister was put under intense pressure. Media coverage, however, dissipated after the BOC contract was cancelled, and two staff members lost their jobs. (see here)
We’re concerned the impetus required to introduce an effective solution may have been lost. So much energy has been expelled laying blame and in a vain attempt to prevent what is an inevitable error – the pipeline crossover.
Despite our best attempts pipeline crossovers will persist throughout the world. Consider for a moment the complexity of piping in any hospital and that ‘To Err is Human’.
We’ve identified numerous cases from a brief internet search. However, as front line staff, we cannot access error databases – see Healthcare: Flying Blind – we’ve little doubt the magnitude of this problem is much greater than represented here (click on images below):












 Italy, 2007.")














The challenge is to accept that despite our best efforts, errors will continue to occur, and yet prevent these errors from leading to adverse outcomes.
‘While most of us assume that “errors = accidents”, aviation knows that “errors – safeguards = accidents”. By obsessing over error reduction (via root-cause analysis), we miss opportunities to increase safeguards. Nick Argall
Ultimately we’re accountable for our own actions, however where work environments can be effectively improved, in the interest of patient safety, they must be.
If the neonates at Bankstown Hospital were resuscitated via an anaesthetic machine it would have alarmed indicating a hypoxic (lacking oxygen) gas. All anaesthetic machines have analysers which continuously assess gas delivery.
If gas analysers were mandated on neonatal resuscitators the staff at Bankstown would have known oxygen wasn’t being delivered. The cost of mandating gas analysers on neonatal resuscitation trolleys would be insignificant compared to liability payments for pipeline deaths. (US example year 1992 alone: US$7,440,000)
Australia has a tremendous healthcare system developing numerous safety innovations (see here). We’re well placed to pioneer safety systems to be emulated by the rest of the world.
Let’s not miss out on this opportunity.
Support the Implementation of Gas Monitoring in Areas of Resuscitation #SIGMAR
2 Comments