
Central lines are essential for the care of many patients, however we estimate at least one patient dies worldwide every day from central line related air emboli. The image above is from a CNN report – one of thousands of similar cases.
All of these cases are avoidable.
Frequently Asked Questions (please click on links in red):
- What is an air embolus and how do they occur?
- How frequently do central line air emboli occur and where is the evidence to support this claim?
- What should we do when a patient requires their central line to be removed but they can’t lie flat?
- This issue persists despite education & policy writing – why is this and how else can we remind staff to remove central lines supine?
- How can we stop those air emboli which occur from accidental central line disconnection?
- How might we reduce air emboli which occur during central line insertion?
- Why hasn’t the magnitude of this issue been recognised before?
Awareness about this issue is poor, and solutions so far implemented have had limited effect. We need to appreciate the complexity of our work environments and apply human factors engineering if we are to prevent these iatrogenic complications.
Help:
The power is in your hands to make a difference. Review and implement these 5 effective solutions:
1. Equipment
2. Vascular Access Decision Tree
3. Centralised Education and Training
4. ‘Remove Central Lines Supine’ animation & screensaver
5. Central Line Management Form

See: Central Line Related Air Embolism – Applying Human Factors to the Design of Safe Systems
You can help right now by signing this petition (see here) which goes straight to sterile dressing manufacturers asking them to imprint a point of care reminder on sterile dressings for central lines which states: ‘REMOVE CENTRAL LINES SUPINE’ ‘TO AVOID AIR EMBOLI’
Frequently Asked Questions:
How frequently do central line air emboli occur and where is the evidence to support this claim?
How frequently do central line related air emboli deaths occur? (see here):
Even the most conservative estimates (5million CVCs per year in US, air embolus 0.1% of CVCs, and 23% mortality) indicate 1,150 deaths per year from this avoidable complication in the US alone. We’ve provided a list of numerous case reports and case series below.
Does education and experience help reduce the incidence? (see here)
Unfortunately studies suggest that those with greater experience may be less likely to follow appropriate procedures to minimise the risk of CVC related air embolus. Also the impact of education tends to wane rapidly with time.
If CVC related air embolus is so prevalent where are all the reports?
Below we’ve collated numerous case series and an overwhelming amount of case reports which highlight the prevalence of this problem. Please note we have no access to error report databases (see here) – these cases represent only some of those available via the internet – we have little doubt there are multiple more.
As is the nature of adverse events in healthcare they tend to be dispersed in time and place. This often starves us of the impetus required to put effective system measures in place.
We’ve only just started to collate this data, however one may already start to appreciate the magnitude of this issue.
Please help us put a stop to these avoidable adverse events: (read here)
Thank you.
Case Series
158 cases of ‘cerebral’ air emboli related to CVC. 21% mortality.
52 of 86 cases of air embolus presenting for HBOT at one institution
15 cases one institution radiology dept in 5 years
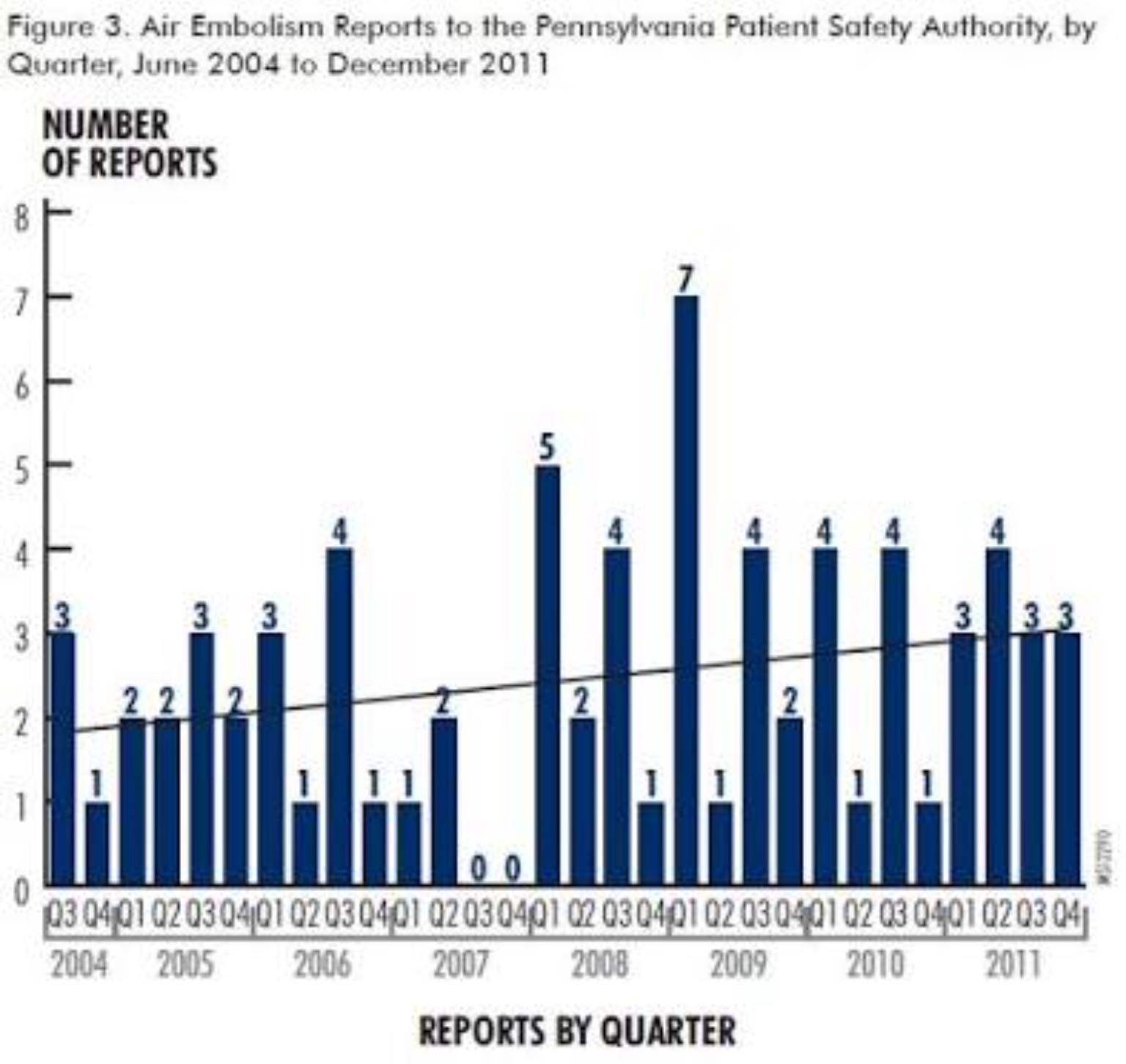
11 reports NPSA UK (2009 to 2011) all on removal of CVC 9 in sitting position
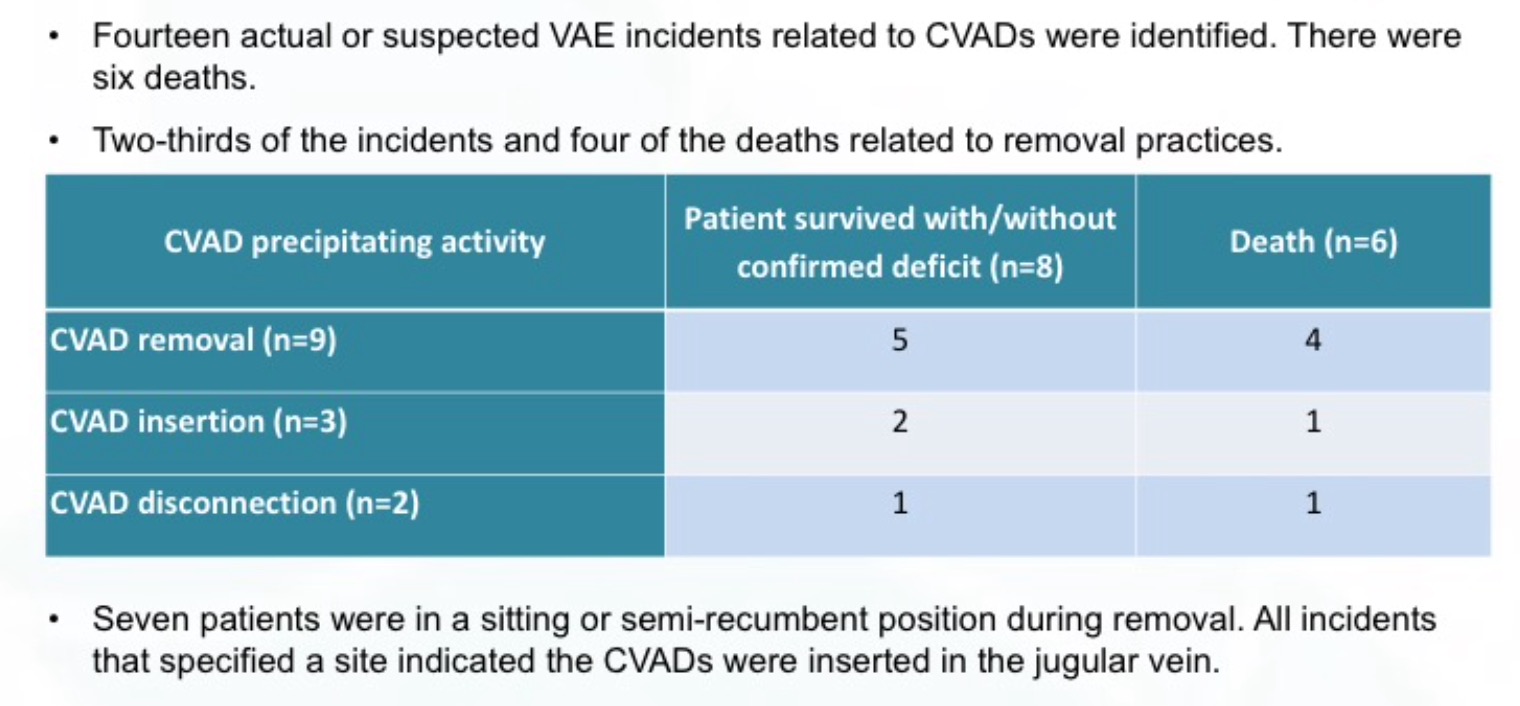
8 reported deaths 51 near miss events NSW CEC since April 2012
6 CVC related air emboli AIMS database
10 cases (4 deaths) air embolus on removal of dialysis catheter
26 patients suffering cerebral air embolus
6 cases related to CVC removal
19 cases of CVC air embolus, 7 fatal
8 cases of air embolism from central line removal
By 1987 total of 79 cases in world literature, 25 (32%) had fatal outcome
2 fatal CVC related cerebral air emboli & literature review
5 cases of CVC related air emboli in lung transplant recipients
Several cases of air embolus related to central lines in NPSA
9 reports NPSA patient deterioration from CVC removed upright
3 reports of harm from CVC being left open to air
2 cases of homonymous hemianopia from CVC related cerbral air emboli
2 cases (one death) post removal of central line
2 paediatric patients air embolus on insertion of CVC
6 patients suffering neurological injury related to CVC management
Median claim for VAE US$ 325,000, 100% payment. 2007 range $25,800 to $4,120,00
85 yr old – cerebral air embolism and death days later
2 cases reported by same practitioner
40yr female air embolus from femoral CVC insertion
72yr male dies post CVC insertion from cerbral air embolus
Air embolus diagnosed on echocardiogram
Echo diagnosis of air embolus with CVC inserted in upright position
Death from air embolus during subclavian venepuncture
66yr female IVC air embolus from femoral CVC
65yr male air emboli during CVC insertion
17yr female died, air embolus post CVC insertion
49yr male death from CVC related air embolus
67yr male air embolus from femoral CVC insertion
Case Reports – Maintenance
Disconnection / ports left open
Death of 29yr old living renal donor transplant recipient
33yr female, 17 weeks pregnant. Child died at 4 months of age.
77yr male cerebral air embolus
66yr female collapsed from CVC ports being left open
62 yr male air embolus from disconnection
Death from sheath disconnection
81yr female death from CVC port being left open
Disconnection of CVC lead to stroke & later death. Over US$18million payment.
65yr male died post CVC disconnection
38yr male air embolus from misconnection of CVC
Fatal air embolism from CVC misconnection
2yr old air embolism from misconnection
Cerebral air embolus from CVC misconnection
81yr male death – air in portacath
72yr male – severe permanent neurological injury post catheter misconnection
Massive air embolus via CVC during ECMO
Other e.g. damage to central line
79yr male dies from cerebral air embolus after lacerating CVC while shaving
71 yr male – severe neurological impairment
52yr male lacerated CVC while shaving
72yr male lacerated CVC while shaving
62yr female air embolus post rupture of CVC
Air embolus from accidental laceration of CVC
Case Reports – Removal
1. Patient not supine
Death
16yr female – CVC removal in preparation for discharge
50yr male – CVC removed in preparation for discharge
53yr male – Dialysis catheter removed, US$10million settlement
Father of 3 – death on catheter removal, US$8.2million settlement
23yr female – US$6million settlement
18yr male death post CVC removal
Death on removal of CVC, patient sat up
65yr male, severe cerebral air embolus ultimately causing death
Lethal pulmonary air embolus on removal of dialysis catheter
Death 8 days post op from CVC removal
Lethal case of air embolus from dialysis catheter removal upright
43yr male death post CVC removal
Male – stroke and death over 2 months later from CVC removal upright
Female (mother) death from CVC removal in upright position
Death from removal of double lumen catheter in upright position
36yr male died post CVC removal
73yr male died post removal of double lumen dialysis catheter
44yr male, Liver Transplant, death post CVC removal
18yr male, Liver Transplant, death post CVC removal
Female, death post removal of CVC
68yr female death post CVC removal
83yr male death post CVC removal in upright position
20yr male death from CVC removal upright
Neurological Impairment
Acute decompensation, CVC removed by resident – review by Dr Peter Pronovost
57yr female minimal long term injury
Female – severe neurological injury, US$3.85million settlement
35yr – central line removed by 1st yr resident, severe injury, US$5.75 million
54yr female – severe neurological injury, US$3.8million settlement
95yr female, permanent neurological impairment
54yr male air embolus and neurological deficit post PA catheter removal
50yr female massive cerebral air embolus and severe neurological injury
Young male air embolus post CVC removal
20yr male – treated with hyperbaric oxygen therapy
43yr male cerebral air embolus from CVC removal
Air bubbles on echocardiography post CVC removal
76yr male stroke from air embolus post CVC removal
23yr male coronary air embolism and MI
57yr female cerebral air embolism post removal of CVC
71yr male CVC removed ’45 degrees head up’
No residual deficit
27yr male 30 mins post removal
73yr male air embolus post CVC removal by House Officer
2. Central line insertion site not sealed sufficiently
51yr old, cerebral air embolism, site not sealed appropriately
49 female stroke post CVC removal
65yr male air embolus post air embolus removal
Near fatal embolism, fibrin sheath as portal of air entry
76yr male air embolus via residual tract
65yr male air embolus post removal – outcome unknown
Please note we have only just started to collate this date. We have little doubt there are hundreds of other individual case reports in journals which are not included above. These reports only represent a fraction of the true number of cases. We will continue to update this list.
Please help stop these avoidable deaths: click here.
Estimates of Frequency:
1. How many central lines are inserted per year?
In US an estimated 6 million lines inserted per year and increasing.
5 million per year in US (NEJM 2003)
More than 5million per year in US. Approximately 8% of hospitalised patients.
As many as 5million CVCs per yr in US. 15% experience complications.
48% of ICU patients. 15million CVC days per year in US.
Estimated 200,000 CVCs per year in NHS (BMJ 2013)
2. What proportion of the central lines are complicated by air emboli?
Incidence may be as high as 0.8% (AAGBI)
0.13% of interventional radiology CVC manipulations
15 of 11,583 radiographically inserted central lines
Gas embolism complicates 2.65 per 100,000 hospitalizations
3. What proportion of the air emboli result in death?
Review of 24 cases – 50% died, of remainder 42% had permanent neurological injury
4 out of 10 cases resulted in death
Awareness, Experience & Education
Survey: Only 31% of nurses (whose job description included removal of central lines) reported using all the recommended procedures. (see here)
Nurses more aware than doctos of risks of air embolism on CVC removal (see here)
Air embolism entirely preventable complication, but not widely known among practitioners (see here)
Are we missing too many cases? (see here)
Nurse Survey. In overall group comparison, few differences were found between nurses and physicians in terms of patient positioning at CVC insertion or removal. Nurses were more likely than physicians to request air-occlusive dressings after CVC removal (19 of 53 [36%] vs. 12 of 140 [9%]; p < .001), but there was no difference between nurses and physicians in awareness of VAE as the reason for choosing one patient position or dressing over another (29% vs. 39%, respectively). Critical care nurses with <=2 years of experience more often placed the patient in the supine or the Trendelenburg position for CVC removal than nurses with >2 years of experience (71% vs. 26%; p = .03).
Although most physicians (127, 91%) chose the Trendelenburg position for CVC insertion, only 42 physicians (30%) reported concern for VAE. On CVC removal, only 36 physicians (26%) cited concern for VAE. Some physicians (13, 9%) reported elevating the head of the bed during CVC removal, possibly increasing the risk of VAE. Awareness of VAE or its prevention did not correlate with the level of physician training, experience, or specialty. After the educational intervention, concern for and awareness of proper methods of prevention of VAE improved (p < .001). At 6-month follow-up, reported use of the Trendelenburg position continued, but concern cited for VAE had returned to baseline. (see here)
What is an air embolus and how do they occur?
An air embolus is basically air in blood vessels. They occur when there is an opening between a blood vessel and the atmosphere (or other source of air) and there is a pressure gradient allowing air to enter the blood vessel i.e. the pressure in the blood vessel is less than that in the atmosphere. Every time we breath in we create a negative pressure in our chest which sucks air into our lungs. The blood vessels in our chest are also subjected to this negative pressure. If there is an opening between blood vessels in the chest and the atmosphere air can open very rapidly. Enough air can enter a central line in a matter of seconds to cause a fatal air embolus.
Central line related air emboli tend to occur from:
1. Accidental line disconnections.
2. During line removal if patients are sat upright.
3. On insertion of larger lines (e.g. Tunnelled Vas Caths) with patients breathing spontaneously, generating negative intrathoracic pressure.
What should we do when a patient requires their central line to be removed but they can’t lie flat?
Patients who can’t lie flat or have other risk factors have an increased propensity for air embolism on central line removal. In these circumstances there needs to be an escalation of procedure:
Assess patient for increased risk of air embolism before removal of the CVC. Risks include:
– Respiratory compromise (can generate a large negative intrathoracic pressure increasing risk and rate of air entrainment. Consider if the patient would benefit from non-invasive ventilation support around the time of central line removal)
– Intravascular depletion (which can lead to a greater negative intravascular pressure, increasing the risk and rate or air entrainment)
– Inability to lie flat for an extended period (if unable to lie flat may create a pressure gradient that favours movement of air into the circulation)
– Low body mass index (smaller tract between the atmosphere and the vessel)
If the patient is unable to tolerate lying in the supine position or are considered high risk, the following should occur:
– Do not remove the CVAD in the first instance
– Contact an experienced critical care medical officer to review and manage the patient
– Delay removal until the risks can be minimised (if possible)
– Vascular access nurse (or experienced nurse) remove central line when appropriate
– Critical care medical officer in attendance
– Ensure alternative venous access already obtained
– Remove line in an adequate environment – monitored, with arrest trolley at hand
– Patient to remain monitored until satisfied risks of air embolism have abated
Beyond education and policy documents how else can we remind staff to remove central lines supine?
Despite education and policies we note that many medical staff still believe that the correct position to remove central lines is with them sat upright:
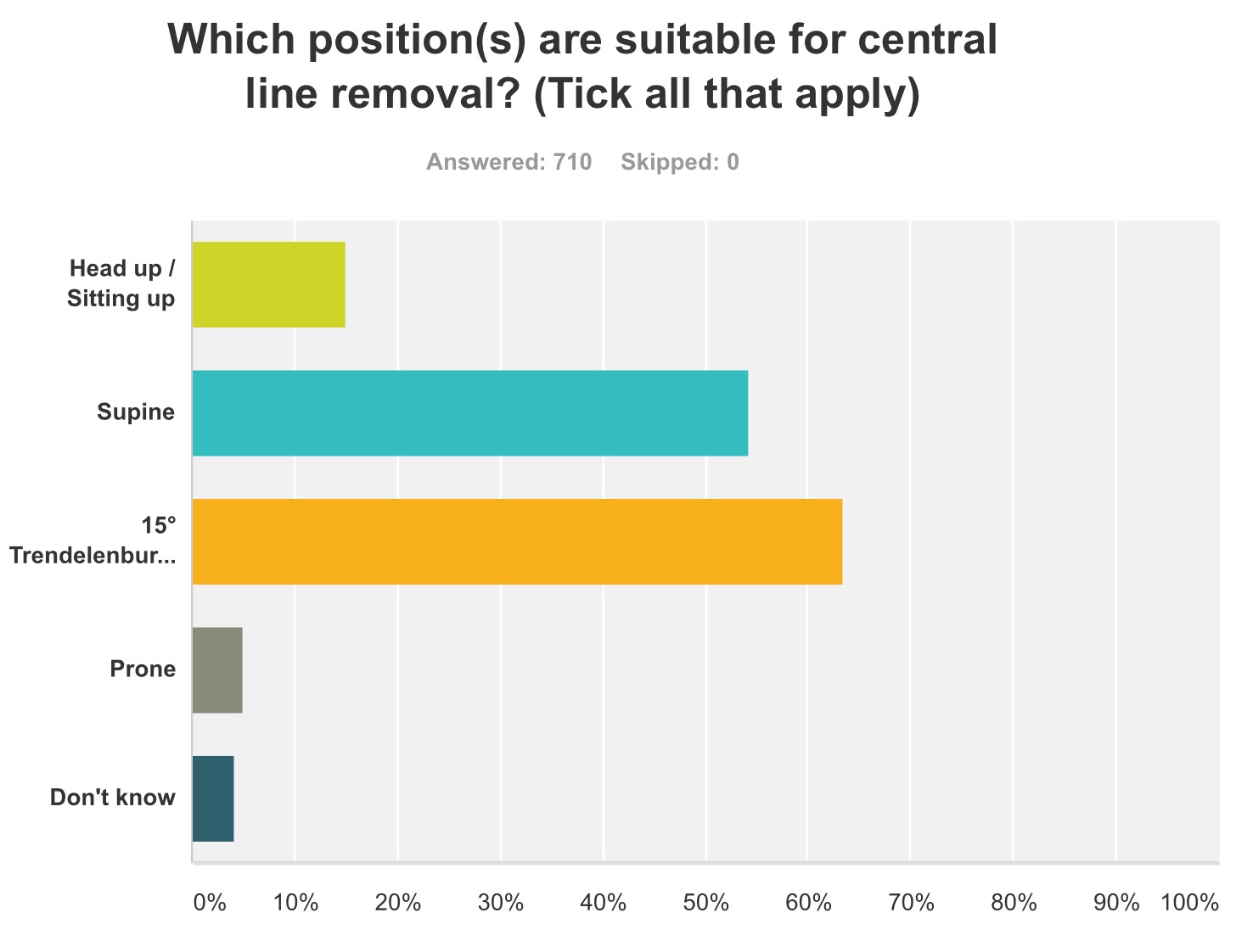
This issue may be explainable through understanding how humans work in systems. Also all healthcare staff will have learnt first aid and that bleeding sites should be elevated above the level of the heart to reduce further bleeding – unfortunately when it comes to a central line sites this puts the patient at grave risk of an air embolus. Further removal of central lines may seem like a benign procedure – perhaps to some posing little risk beyond removing a peripheral cannula. Given central line air embolus error reports are siloed away in reporting systems many front line staff have not even heard of this issue.
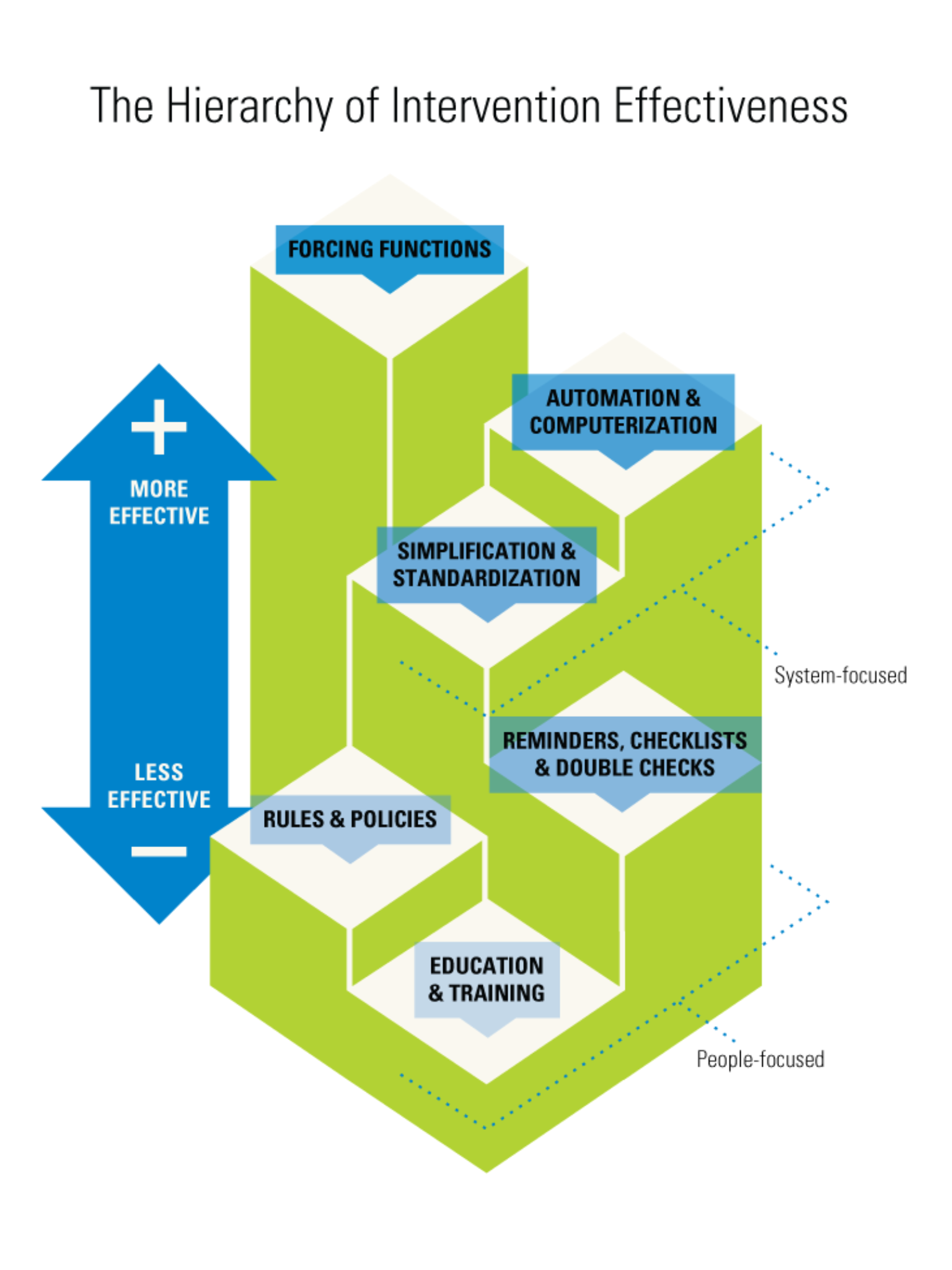
The human factors diagram below neatly depicts that education and policy writing, interventions we have relied heavily on in healthcare are actually relatively inneffective when it comes to improving safety. To learn more about human factors please click on the resources link.
We are in the final stages of releasing an animation focused on a simple message:
‘REMOVE CENTRAL LINES SUPINE’
We have liased with several central line dressing manufacturers to develop dressings with the phrase ‘Remove Central Lines Supine’ ‘To avoid air emboli‘ imprinted on them as a point of care message to staff. Perhaps this is the best location to have a point of care message without interfering with the day to day management of the central line.
Please sign this petition (click here) which goes straight to staff working for the major sterile dressing manufacturers who can make this happen.


How can we stop those air emboli which occur from accidental central line disconnection?
Air can enter central lines accidentally left open to air in a matter of seconds causing intractable cardiac arrest. There have been numerous case reports of deaths from this mechanism – all are avoidable.
We do not need central lines or vascular attachments that open to air. We could effectively eliminate this risk by replacing them with those that do not.
We will continue to update information on suppliers as it becomes available.
Please note we have no financial interest with any of the products discussed on this website.
Equipment Suppliers
Central Lines:

Altius central lines – TGA approval granted October 2016
Bill Houghton National Product Manager – Business Development
Regional Health Care Group,
Mobile: +61 (0)426 227 207
Email: bill.houghton@regionalhealth.com.au
Stopcocks:

Paul Williams – Director New Medical, Mobile: +61 (0)410 537746
Email: sales@newmedical.com.au
Stopcock with moulded H-Port valves product 50.262H
TUTA Australia, Vesna Acevska, Phone: 1300 361 162
Email: info@medaust.com
How might we reduce air emboli which occur during central line insertion?
The risk of air emboli on central line insertion may be reduced by ensuring the patient is in a head down position, and where appropriate using positive pressure ventilation (keeping the intrathoracic pressure greater than atmospheric pressure).
Tunnelled Vas Cath central lines appear to be at particular risk of air emboli on insertion.
Why hasn’t the magnitude of this issue been recognised before?
Many front line staff healthcare staff have not even heard of deaths occurring from Central Line Related Air Emboli:
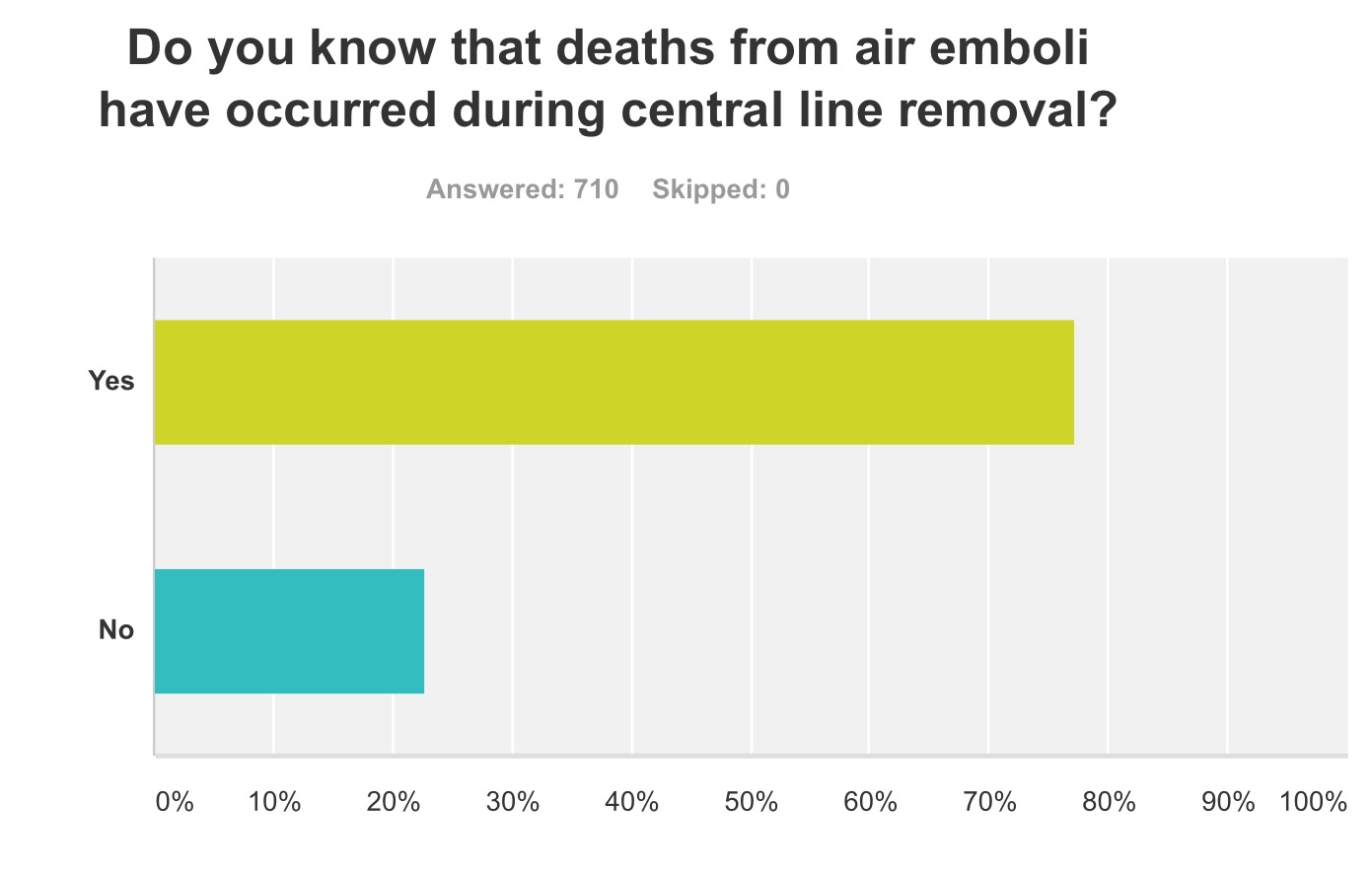
Unfortunately the construct of error reporting systems worldwide leads to vital information being siloed away. Current error reporting systems lack transparency (see here).
Medical error has been reported as the third greatest cause of death in hospitals (see here). The risk of central line air emboli is only one of thousands of hazards. If we are to overcome these unnecessary risks we will have to change the way we manage healthcare safety (see here).
4 Comments