In Australia, 2016 was marred with the events which occurred at Bankstown Hospital (see here).
More deaths have occurred because of accidental hospital gas pipeline cross-overs. (To read about cases click on each image box below):












 Italy, 2007.")














In Australia, 2016 was marred with the events which occurred at Bankstown Hospital (see here).
NSW Health should be commended on the publication of their recommendations following the tragedy.
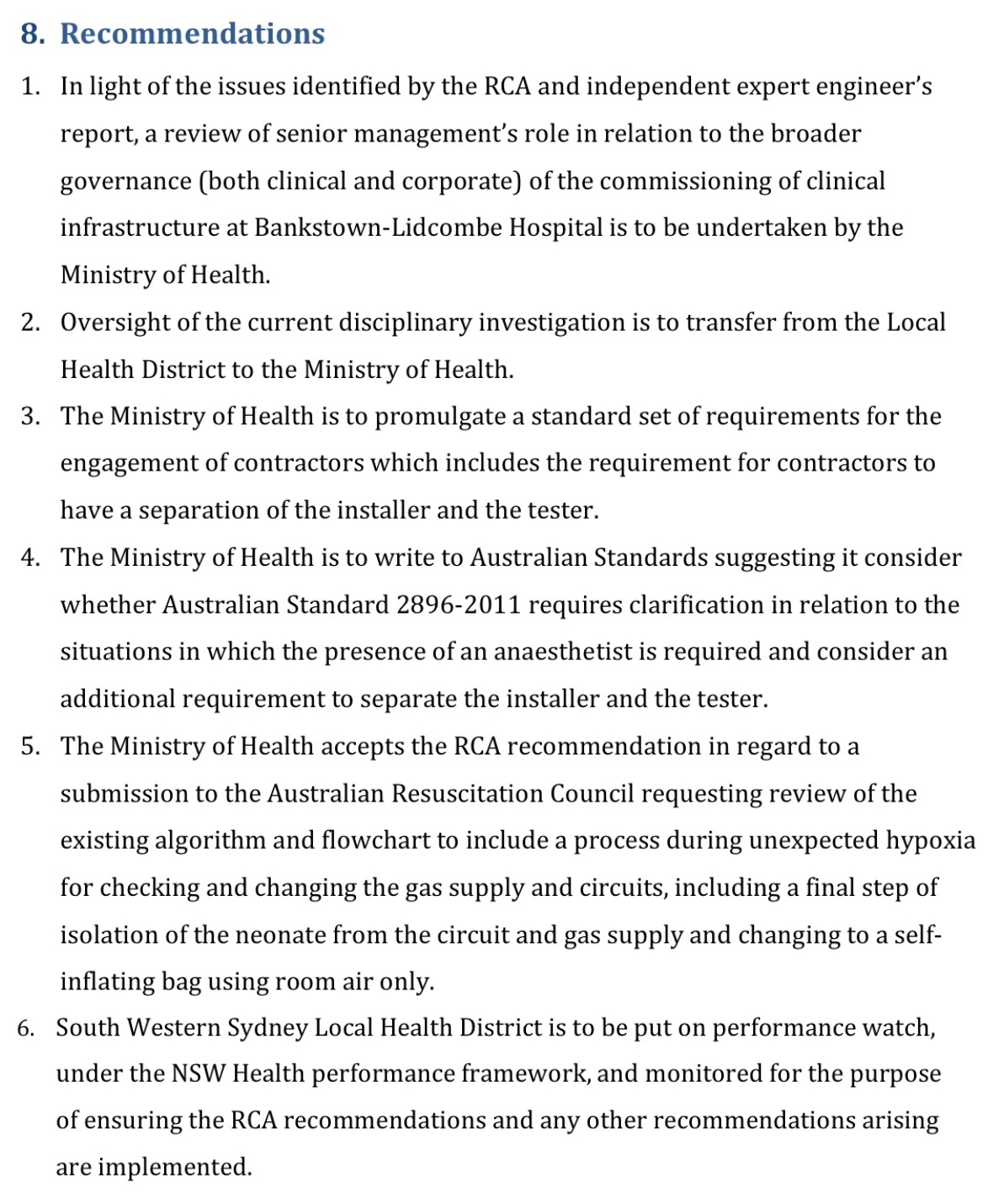
It is useful to identify those involved, the procedures used and assess why errors were made. However consider for a moment the complexity of gas pipelines in hospitals, the frequency of maintenance procedures, and that pipeline crossovers have occurred in areas considered unaffected by renovation. Would other individuals under similar circumstances make the same mistake?
It is wise to review existing policies, to ensure they are watertight. However, given pipeline errors continue despite historical policy changes, how much impact will further policy change have on preventing future pipeline cross-overs?
There may be merit in considering changes to existing resuscitation guidelines. However note that newborn resuscitation commences on air, oxygen being introduced when the newborn deteriorates. How likely is it that a clinician would remove presumed oxygen for the same reason they’ve commenced it? It may be worthwhile assessing this proposal through simulation before its introduction?
Unfortunately, on review, the NSW Health recommendations may do little to prevent similar adverse events in the future. Similarly, despite previous efforts worldwide, pipeline crossovers have persisted. That we may not hear of a similar case in NSW for some time will likely reflect that adverse events are dispersed in place and time.
The challenge is to accept that despite our best efforts, errors will continue to occur, and yet prevent these errors from leading to adverse outcomes.
By obsessing over error reduction (via root-cause analysis), we miss opportunities to increase safeguards. ‘While most of us assume that “errors = accidents”, aviation knows that “errors – safeguards = accidents”. Nick Argall
Where safeguards can be introduced and work environments effectively improved, in the interest of patient safety, they must be.
Neonatal resuscitation trolleys lack gas analysers. If the neonates at Bankstown Hospital were resuscitated via an anaesthetic machine it would have alarmed indicating a hypoxic (lacking oxygen) gas. All anaesthetic machines have analysers which continuously assess gas delivery.
If gas analysers were mandated on neonatal resuscitators the staff at Bankstown would have known oxygen wasn’t being delivered. The cost of mandating gas analysers on neonatal resuscitation trolleys would be insignificant compared to liability payments for pipeline deaths. (US example year 1992 alone: US$7,440,000)
Australia has a tremendous healthcare system developing numerous safety innovations (see here). We’re well placed to pioneer safety systems to be emulated by the rest of the world.
Let’s not miss out on this opportunity.
Support the Implementation of Gas Monitoring in Areas of Resuscitation
One Comment