
Last year the BMJ reported medical error as the third greatest cause of death in healthcare.
Does the design of error reporting systems render them powerless to change this?
Current systems are designed using a command structure:
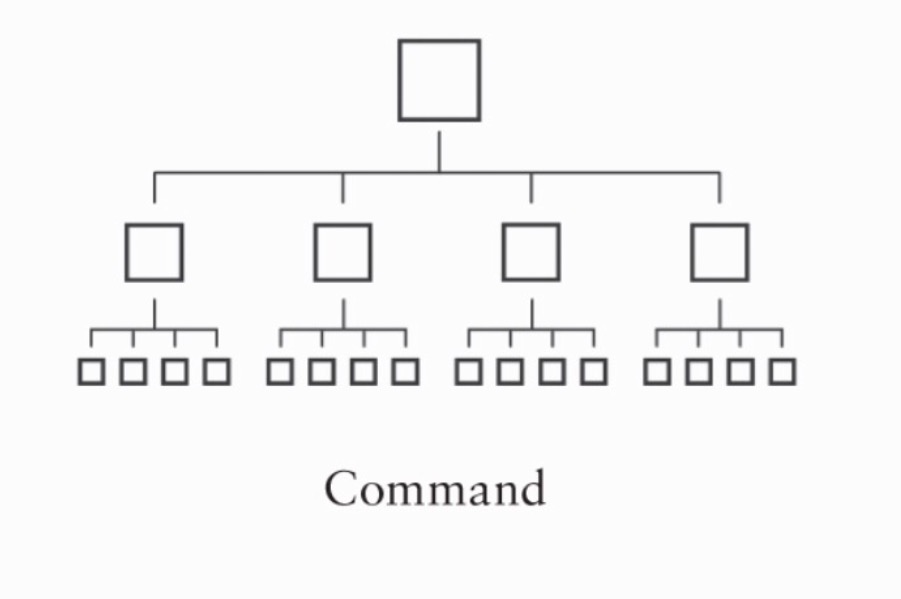
Command structures have been present for hundreds of years and were used with great effect to improve efficiency during the industrial era. However they only work when those in charge actually understand how everything will interact.
Healthcare work environments have become so complex that it’s impossible for those at the top to truly understand the nuances of front line work.
Perhaps the ability to predict the outcome to an intervention is what separates an issue which is merely complicated from one which is complex.
For example if staff continue to pour antiseptic solutions into unlabelled gallipots despite a policy dictating otherwise this is a complex problem.
With so many interactions at play, one cannot reasonably forecast the output based on the input (the policy). In this case interactions include staff turnover, limited access to the policy, historical practices, lack of access to sterile labels, poor awareness of adverse events, time pressure…..
You cannot force the complex to merely conform to rules meant for the complicated.
Further, the command structure of current error reporting systems secludes vital information.
An error which occurs at hospital or department ‘X’ cannot be learnt from by those in hospital ‘Y’. It can only be shown to other parties if released by those at the top on a ‘need to know’ basis. The problem with this logic depends on the assumption someone actually knows who does and who doesn’t need to know what.
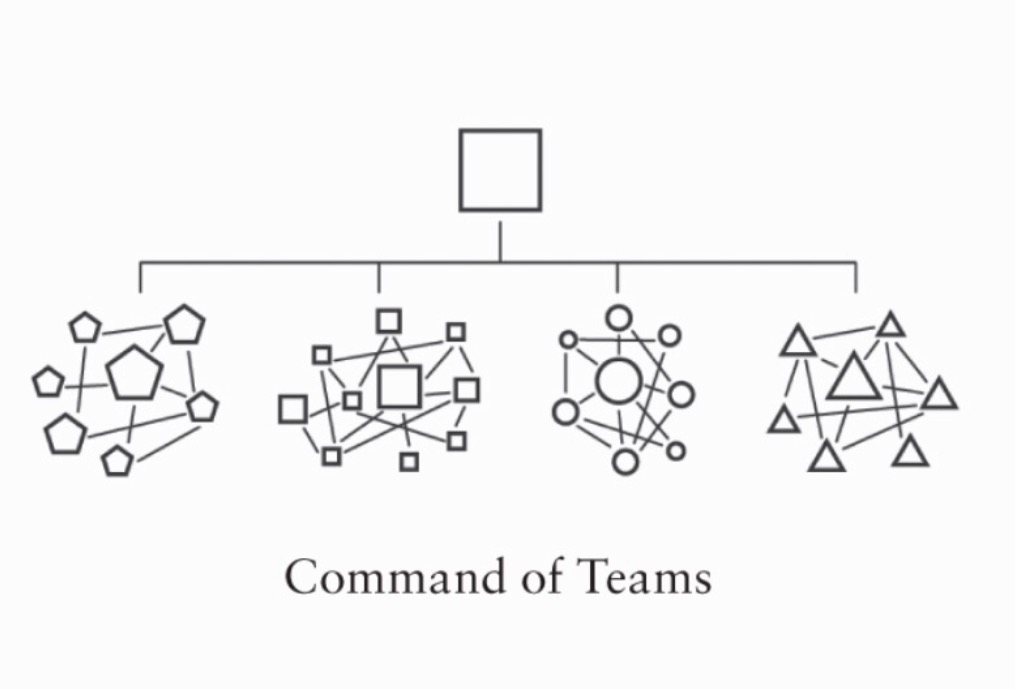
Competition between departments and hospitals has been used in the past to help drive improvement – in effect generating a ‘command of teams’. However competition stifles cooperation and inhibits the valuable sharing of information.
If we remove a hazard at one institution are we not morally obliged to remove it elsewhere?
How we organise structure says a lot about how we think people behave, but how people behave is often a by product of how we set up structure.
Error reporting systems, through their command design send out a message that error information is to be secluded.
We become more concerned with how best to control information than how best to share it. This culture permeates throughout healthcare. As a result dispersed information about adverse events becomes even more scarce and much less impactive.
That there are no systems for reporting hazards conveys a message front line staff should just put up with their work environments.
As healthcare stands few will be criticised if we maintain the status quo, keep quiet about the hazards yet present the adverse events which occur because of their presence into inneffective opaque reporting systems. As a result the same adverse events repeat again and again and again.
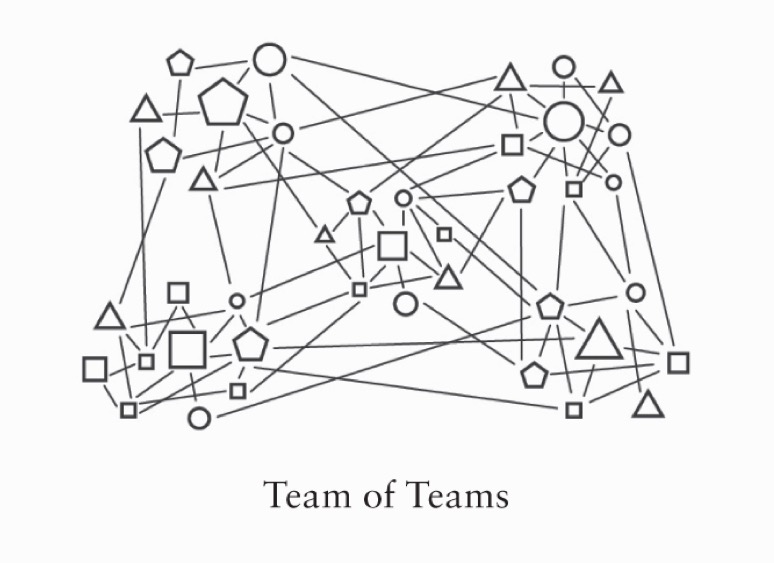
Healthcare safety would benefit from a transparent de-identified medical error and hazard reporting system which generates networked teams to conceive effective solutions. Progress made on generating these solutions should be available for everyone to see.
Greater transparency about what is being done to achieve a goal is a massive boost to morale.
Solutions should be developed by those most likely to understand what will be effective – front line workers and human factors engineers working in teams with others from numerous backgrounds.
The role of those currently at the top of command structures needs to change. They need to develop an ‘eyes on hands off’ approach, where they can view everything that is happening, provide support where it is needed, request more information to help guide decisions and supervise processes. Their role should no longer be one of controlling puppet master but rather that of an empathetic crafter of culture.
We all want the best for patients. Let’s provide frameworks to deliver this, frameworks where anyone is able to drive improvement kept in check by others.
In empowering those on the front line, solutions will come more quickly, their quality will be greater and they will be much more effective.
For patient safety to improve we’ll need to become a ‘Team of Teams’.
Much of the text of this post has been adapted from ‘Team of Teams’ by General Stanley McChrystal et al – we highly recommend you read it.
Below we discuss several ‘command’ solutions (click on links in red) in response to error reports. They’ve been developed by those at the top of command structure error reporting systems.
Within the command structure everyone is doing the right thing – front line staff are reporting an adverse event, the adverse event is being entered into a secure error database, the information is reviewed by the custodians of the error report information who work diligently to develop a solution. This solution is then passed back down to the front line. Everyone has done right thing within the command structure however nothing has been done right – the solutions have minimal if any effect on the front line.
We provide alternative effective solution which we hope to deliver.
Command Solution – Reminder for staff to clamp off central lines to avoid air emboli
Effective Solution – Only use central lines which don’t open to air
Command Solution – Policy to inhibit re-spiking of IV fluid bags to prevent air emboli
Effective Solution – Use only IV fluid bags which don’t entrain air when disconnected
Command Solution – Safety notice
Effective Solution – Ban Indistinct Pourable Chlorhexidine
Command Solution – Proposals to Gas Pipeline Mix Up
Effective Solution – Use of gas analysers in resuscitation areas
Command Solution – Alert about hazardous Draeger APL valves
Effective Solution – Recall Draeger APL valves
Command Solution – Admonish hospital staff for not maintaining dental drills
Effective Solution – Use only dental drills which cut out if they heat up
We’ve chosen these examples to help illustrate the problems with patient safety. All of these unnecessary hazards (and thousands more like them) still exist within hospitals throughout the world. While we have command structures of error reporting they will persist. We’re working to remove them and creating great networks for future progress.
The patient safety machine is broken – perhaps it’s design and the increasing complexity of our work environments meant it could never work.
We’re excited with the prospect of developing a network to drive effective patient safety improvements.
You can help and we would very much appreciate your input. Please get in touch.
2 Comments